
A New Insight to Mysterious Talmudic Rulings:
Metzitza and Bathing in Warm Water in the Performance of Jewish Ritual Circumcision
A modern Explanation for Their Institution
and its Clinical, Halachic, and Legal Significance
Mordechai Halperin, M.D.
David Fink, Ph.D.
David Rosen
* Presented as the fifth annual Jakobovits Memorial Lecture, January 2005, London, UK.
Contents
- Circumcision: Epidemiological Background
- Mohalim and Physicians
- Inheritance of Hemophilia
- Hypospadias Hidden by a Complete Prepuce
- Haemolytic Anaemia in the Newborn
- The Mystery of Metzitza
- The Mystery of Bathing in Warm Water
- Location-Dependent Health Risks
- The Shulchan Aruch R. Moshe Isserles
- Four Questions
- A Physician’s Testimony in the Jerusalem district Court
- Anatomy of the Normal Penis
- Hypospadias
- The Solution of the Mystery of Bathing in Warm Water
- Post-Circumcision Hypoxia in Israel
- Erroneous Medical Reports
- Legal Significance
- The Medico-halachic Significance
- The Solution of the Mystery of Metzitza: Why Metzitza was instituted
- Circumcision: Epidemiological Background
Israel. Circumcision is performed as a religious obligation for approximately 100% of Jewish males and for more than 90% of Muslim males. Although in the distant past circumcision was performed only for religious reasons, since the Second World War millions of babies (60%-90% of the males born in the U.S.2) have been circumcised for medical and cosmetic reasons.3 Among the most striking medical advantages of circumcision is the dramatic decrease in the incidence of cancer of the penis. An editorial in the New England Medical Journal, the most widely circulated medical journal in the world, summarised the protection against cancer of the penis afforded by circumcision:
“Furthermore, circumcision reduces the risk of penile cancer. In uncircumcised men, the lifetime risk of this cancer is about 1 in 500, as compared with a risk of 1 in 50,000 to 1 in 12 million in circumcised men.”4
Circumcision, is the most common surgical procedure performed on males in America[I] [II] and
In other words, an uncircumcised man has between 100 and 24,000 times greater risk of developing penile cancer than a circumcised man. Epidemiological data indicate around 11,000 deaths of uncircumcised males in America due to cancer of the penis over the last 45 years.'’ It follows that circumcising the general population in the United States can prevent over 10,000 deaths due to cancer of the penis over the next 50 years.
While circumcision is not an absolutely riskfree procedure, the risks are very minimal. In the past 45 years, there have been only 4 (!) deaths in America from complications of this surgical procedure. When we consider the 10,000 lives saved from this procedure, the benefits are clear.
The Sages were quite aware of the potential dangers associated with circumcision. Therefore, they established medical guidelines imbued with halachic status for the purpose of minimising the risks. These guidelines include detailed instructions regarding the circumcision procedure from its preparatory stages through the surgery itself, postoperative follow-up, and treatment.[5] [6] Prerequisites regarding the patients’ health and other necessary conditions for the procedure were also specified.
Maimonides’ halachic-medical guidelines are typical:
Only a newborn who is free of disease is circumcised, for danger to life supersedes everything; circumcision can be delayed, but it is impossible to restore the life of a baby.[7] [8] [9]
Indeed, during times of religious persecution there is a special commandment of sanctifying the name of God. For example:
‘To those who love and keep my commandments’ – these are they who dwell in the Land of Israel and offer their lives for the fulfilment of all the commandments.
Why do they execute you? Because I circumcised my son. Why do they burn you? Because I learned Torah diligently. Why do they crucify you? Because I ate unleavened bread. Why do they whip you? Because I took the palm branch. 9
But outside the times of religious persecution, it is prohibited to perform a circumcision in a life threatening situation, as made clear by the Talmud and halachic authorities.
Mohalim and Physicians
Over the last few thousand years this most common surgical procedure has usually been performed by mohalim, not physicians. As an interesting anecdote it should be remembered traditions a Jewish mohel, rather than the royal physician, was called to perform circumcisions for the royal family in England.[10] [11] As reported in the press, the circumcision of Crown Prince Charles took place in Buckingham Palace and was performed by Rabbi Yaakov Snowman, the official mohel of the London Jewish Community.11
In the United States, where the majority of newborns are circumcised even though they are not Jewish, most of the procedures are performed by physicians. In Israel, on the other hand, where the tradition of circumcision did not begin in the 20th century, over 99% of the circumcisions are performed by experienced mohalim. In recent years there have been rumours of attempts to transfer the responsibility for circumcision from the mohalim to physicians. Despite such widely publicised attempts, there are still only few
physicians with practical experience in performing circumcision in Israel. The experienced mohalim continue the ancient tradition whilst employing modern pharmacology combined with traditional wisdom which has been passed on through the generations.
As a result of their vast experience garnered over the years, mohalim have assembled much medical knowledge as seen in the halachic literature. Some of this knowledge first became known to the medical community hundreds of years after it had been in use by mohalim. Some of it is still absent in medical literature today. An interesting example is the understanding of inherited haemophilia: the Sages perceived the principles of genetic inheritance of this disease around 1500 years before the medical community.
Inheritance of Hemophilia
Excessive blood loss is the main life-threatening risk factor for circumcision. Bleeding is a serious concern for someone with a blood clotting disorder. The most common example of such a disorder (1:10,000 average occurrence[12]) is type A Hemophilia. A hemophiliac can easily bleed to death from a cut or wound. Before the advance of modern medicine, the condition might only have been recognized when the baby bled to death from a circumcision.
Type A Hemophilia is a genetic disorder with a recessive, single-gene, sex-linked inheritance. It causes a deficiency of functional plasma coagulation factor VIII. In general, women with this gene on one of the X chromosomes are asymptomatic carriers of the illness, while their male offspring who inherit this faulty X chromosome develop the illness. In 1784, an American doctor named Fordyce published the first report of observations on the familial transmission of hemophilia[13]. And in 1803, John Conrad Otto (1774-1844) offered the first clear medical description of the illness.[14] [15]
In contrast to this relatively recent understand its inheritance, the Babylonian Talmud (compiled in the sixth century) and understanding of hemophilia and subsequent halachic literature (Maimonides,[16] Meiri,[17] [18] and R. Moshe Isserles – Ramah13), identify a method of transmission for this dangerous affliction – from the mother to the son.[19] With this novel observation,[20] the sages initiated a law that forbade not only circumcising a baby whose brothers had died from a Brit Milah, but also a baby whose cousins from his mother’s side had died following a circumcision.[21] They feared that his maternal cousins carried this inherited disorder and that therefore he was at a significant risk of dying from the procedure.[22]
Hypospadias Hidden by a Complete Prepuce
A further example of medical information which was previously known to mohalim and only recently incorporated in modem medical literature involves the rare phenomenon of hypospadias[23] hidden by a complete prepuce. Until less than 30 years ago, it was generally accepted in medical literature that hypospadias occurs only with an incomplete prepuce. At the end of the 1980s descriptions of this pathological condition began to appear in medical literature,[24] whilst halachic literature had mentioned the phenomenon over 100 years earlier.[25]"’ In addition, mohalim had for generations transmitted an oral tradition regarding this condition. Thus, this rarely occurring penile birth defect offers another example of medical knowledge that was known to the traditional mohel, but only recently realized in the medical community.
Newborn Anemia Due to Hemolytic Jaundice
A newborn hemolytic disorder occurs when antibodies from the mother destroy the fetus’s red blood cells by diffusing from the maternal blood stream through the placenta and into the fetal blood. This is the most common cause for newborn anemia (a deficiency of red blood cells). In the majority of cases, a newborn hemolytic disorder is caused by a mismatch between the mother and the fetus for the presence of Rh antigen D on their red blood cells (RBCs), or a mismatch in their blood types. In rarer cases, it is caused by a mismatch in other antigens found on RBCs.[26] The pathological mechanism is as follows: some of the fetal RBCs pass into the mother’s circulation. These fetal RBCs have surface antigens never before “seen” by the mother. Her immune system considers the surface antigens to be part of a foreign entity and she thus forms antibodies against these foreign antigens and any RBCs that express them on their surface. Passing through the placenta, these antibodies cause massive destruction of the fetus’s RBCs, which can even continue a few days after the baby is bom. The substantial breakdown of the RBCs causes the newborn’s plasma bilirubin to increase at a greater rate than the ability of the newborn’s immature liver to metabolise and excrete it. As the plasma bilimbin rises, the newborn’s skin and conjunctiva develop a more yellow coloration, which is called jaundice. When the RBC breakdown also outpaces the production of new RBCs, he/she has anemia as well. Therefore, newborn jaundice is a clear warning sign of the possibility[27] of a newborn hemolytic anemia.
The connection between newborn jaundice and newborn hemolytic anemia first appeared in the Babylonian Talmud[28] in the context of threats to the life of a baby circumcised prior to the resolution of the anaemia, hundreds of years before any recorded report in the medical literature:[29]
“Rabbi Nathan said… Once I was going to Kaputkia. A woman came before me who had circumcised her first son who died and her second son who died. She brought her third son before me. I saw that he was yarok [yellow[30]]. I examined him, but did not find ‘circumcision blood.’ I said to her: wait with him until he is full-blooded. She waited with him and than circumcised him and he lived. They called him ‘Nathan’ after me.”
Rabbi Nathan describes two stages in his diagnostic observations:
- A diagnosis of newborn jaundice: “I saw that the infant looked yellow.”
- A diagnosis of anemia: “I did not find ‘circumcision blood.’”
Following this diagnosis, Rabbi Nathan instructs the woman to wait and not perform the circumcision until his anemia had subsided, “wait until he is full-blooded.” The woman followed Rabbi Nathan’s recommendations and her son was circumcised at a later time, thereby avoiding the lethal complication that killed his brothers.
The Mystery of Metzitza
Among the obligations of the mohel is metzitza – sucking the area of circumcision immediately after the foreskin is removed. In the Mishna[31] The Sages did not specify the details of the procedure. But one of the mediaeval authorities, Rabbi Yaakov ha-Gozer[32] gives specific instructions:[33]
“Metzitza… How? After the incision and splitting the membrane, one immediately brings the penis into his mouth and sucks the blood with all one’s strength.”
Physiologically, metzitza of the distal portion of the penis applies a negative pressure on the tissue and blood vessels of the glans penis34 35 (the head of the the pressure gradient
penis), thus increasing between the blood vessels at the base of the penis and those at the glans. The clinical significance of raising this pressure gradient will be discussed in Section 19 below.
The Talmud makes clear that the obligation to perform Metzitza derives from medical considerations and is intended to prevent danger:[34]
Rav Pappa said: A mohel who does not perform Metzitza endangers the baby and is dismissed.
Is this not obvious? Since we desecrate the Shabbat for it, it is obviously a danger [and thus it is proper to dismiss someone who fails to do so. What is Rav Pappa’s statement adding for us?].
You might say [had Rav Pappa not made this statement] that this blood is stored up [so sucking it out is not a desecration]. Now we have learned [from Rav Pappa] that the blood is the result of a wound [thereby sucking it out is desecrating the Sabbath],
So sucking is like a bandage and cumin. Just as when one does not apply a bandage and cumin there is danger, so here too if one does not perform Metzitza, there is danger.
Maimonides followed this opinion:36
“How is the circumcision performed? The foreskin covering the glans is cut off until the entire glans is revealed. Afterwards, the soft membrane that is beneath the skin should be split along the midline with one’s nails and peeled back to either side until the flesh of the glans is revealed. Afterwards, one should suck the place of circumcision until the blood in the further reaches will be extracted, to avoid any dangerous situations. Anyone who does not perform this metzitza is removed from his position. After the metzitza is done, he should apply a bandage, a compress, or the like.”[35]
The same reasoning leads to the decisions of the Shulchan Aruch[36] and the Hochmat Adam.[37]
Unfortunately, the Sages never clearly recorded how metzitza reduces the risks of a circumcision. As a result, over time, we have lost the medical information which led our Sages to require metzitza.[38] In the 19th century, some members of the medical community began to raise dissenting voices against metzitza. There were three main arguments proposed against it:[39]
- Absence of known medical indication for
- Risk of the mohel infecting the baby.
- Risk of increased haemorrhaging due to
The first claim regaring the absence of medical indication for metzitza was strongly rejected. This is especially since those who made the objection did not know the Sage’s original medical reason for metzitza. We should remember that not only pure faith in the Sages leads to rejection of this claim, rational evaluation based on the experience of generations also leads to its rejection.[40] The history of medicine shows that the Sages examined medical findings with a critical eye and did not blindly follow Aristotelian doctrines.[41] Therefore, for example, they insisted that the father also contributes to the child’s innate traits in opposition to the thinking of the Greek science.[42] [43] In addition, the Sages record knowledge of pathological anatomy almost 1500 years before the creation of the field,43 and they recognized pathological phenomena regarding circumcision hundreds of years before modern medicine even began to document them.[44] [45] Therefore, it is reasonable to assume that when the Sages claimed their argument they were basing this claim on a rational medical benefit of metzitza.
The medical community’s second argument regarding contamination of the wound was accepted as a valid concern. Consequently, three
fundamental approaches for preventing this risk of infection have developed: strictly maintaining the health of the mohel f cleansing the mouth with an antiseptic (an anti-bacterial substance, like alcohol or wine[46]); sucking through a sterile glass tube, instead of having the mouth touch the penis.[47] [48]
Finally, the objection that Metzitza is liable to increase haemorrhaging at the site of the incision has been rejected on the basis of medical reasons because the bandage and the ‘cumin’ mentioned in the Mishna or ‘powder remedy which stops the bleeding’ as mentioned in the Shulchan Aruch adequately prevent continued bleeding. Since these are applied immediately after Metzitza under the full supervision of the mohel, the slight increase in bleeding was not considered a cause for concern.
So the procedure of Metzitza is still followed today although the mystery has not yet been solved: what was this well-known presumed risk that metzitza avoided, and what is the biological mechanism that will clarify its medical benefit?
- The Mystery of Bathing in Warm Water (Rechitza B'ehamin)
The Mishna'0 considers rechitza b’ehamin, or bathing the baby in warm water, before and after the circumcision (and according to Rabbi Elazar Ben Azarya on the third day post-circumcision as well) to be vital for the child’s recuperation. So much so, that the baby must be bathed in hot water on the Sabbath, even if the water has to be heated specifically for this task on the Sabbath. The Talmud summarizes it as follows:"’1
“The halacha is in accord with Rabbi Elazar ben Azarya in respect to both hot water heated on Shabbat and hot water heated before Shabbat, whether for bathing the whole body or for bathing the area of circumcision, because [not bathing him] it is dangerous for him.”
In other words, the Talmud considers refraining from bathing the baby in warm water before and after circumcision to be life-threatening for the baby. It is certainly clear from a medical standpoint why bathing the baby in warm water would be necessary before the circumcision. Since the days of Semmelweis”2 in the middle of the 19th century, modern medicine has recognized the importance of proper hygiene, which calls for sufficient cleanliness before any surgical procedure. However, not only does there seem to be no medical reason to suggest bathing the baby immediately after or a few days after the circumcision, it is also a bewildering request. Any junior resident in general surgery knows that a fresh surgical wound should be kept away from external moisture for the first few days. If the wound is in contact with external moisture too early, infectious agents may penetrate the wound, which can be particularly dangerous when the postoperative patient’s immune system is not optimally working.
An eight-day-old baby does have a fairly good immune system due to the antibodies he receives from his mother. His ability for relatively fast growth also assists him in recuperating rapidly. However, we are still bewildered as to why the baby must be bathed in hot water immediately following, and a few days after, the surgery, when there is no apparent health benefit. Considering the fact that medical halacha in the Mishna and Talmud was based on the experience of generations, it would be worthwhile researching the scientific basis of such experience which, over many years, indicated that bathing the infant after circumcision has medical justification
- Location-Dependent Health Risks
Maimonides, who was well known as an experienced physician, records in Hilchot Shabbat" that the permission to heat water on the Sabbath for post-circumcision bathing is related to the baby’s life-threatening situation:
“One bathes the child on Shabbat on the day it is born after severing the umbilical cord, and one uses even hot water which was heated on Shabbat, because he would be in danger without this. One salts and wraps him. Because of danger one similarly bathes him prior to circumcision and on the third day after circumcision in hot water which was heated on Shabbat.”
Unfortunately, Maimonides provides us here no medical explanation for the Sages’ instruction regarding bathing after circumcision. In other words, the medical basis for bathing after circumcision is still shrouded in mystery. Further study of Hilchot Mila by Maimonides”4 reveals that in his opinion the medically indicated bathing after circumcision is not a constant imperative, but something that is dependent on the location in which the baby was born.
“In a place where the practice is to bath a newborn, one ought bathe him before and after the circumcision [even] on Shabbat on the day of the circumcision, or on the third day after the circumcision which falls on Shabbat; whether it be bathing his whole body or bathing the area of circumcision; whether it be hot water that was heated before Sabbath, or hot water that was heated on the Sabbath, because of the danger to the child.”
Maimonides, Hilchot Shabbat 2:14.
Maimonides, Hilchot Mila 2:8.
Defining the medical danger to the child as depending on location adds a new dimension of mystery to the medical indication of bathing and creates an interesting situation of different practices in different places. Around 350 years later, similar (though not identical) geographical distinctions were clearly formulated in the halachic decisions of R. Yosef Karo in the Shulchan Aruch and R. Moshe Isserles (the Rama) in his commentary thereupon.
The Shulchan Aruch vs. Moshe Isserles
In the place where the Shulchan Aruch was written, they bathed the infant after circumcision neither during the week nor on Shabbat. R. Yosef Karo was unfamiliar with any places where in his time there existed a medical indication for bathing the infant after circumcision. Thus he wrote:[49]
“In the days of the Talmudic Sages, it was dangerous for the newborn if he was not washed in hot water before the circumcision, after the circumcision, and on the third day following the circumcision. Therefore, they called for this practice to be done on the Sabbath as well. But, nowadays, we don’t have the practice of washing the circumcised child at all, [even on weekdays]. Therefore the law of bathing the newborn on Shabbat is the same as the law of bathing anyone else”
In the location of R. Moshe Isserles, on the other hand, there was nonetheless a medical recommendation to bathe the infant after circumcision although this indication was not absolute. Therefore, it was in general not permitted to violate Shabbat for it. Thus R. Moshe Isserles added this comment to his gloss of the Shulchan Aruch:
“Gloss: In these lands we bathe him [on Shabbat] before circumcision using hot water which was heated the previous day and after circumcision [on Shabbat] we bathe him on Saturday night. Similarly, if the third day after circumcision falls on Shabbat and he seems to need bathing, we prepare hot water before Shabbat and bathe him on Shabbat.”[50]
In his conclusion, however, R. Moshe Isserles added a significant halacha establishing the possibility of cases in which one can determine danger to the circumcised baby by visual inspection
(!). Such danger is an absolute indication for bathing on Shabbat even if violation of Shabbat should be required. This is R. Moshe Isserles’ conclusion.
Moshe Isserles then makes a very significant point. He adds that in some cases one can determine the newly circumcised infant has developed dangerous complications through mere observation (!), and in such a case one should forego the laws of the Sabbath to use the therapeutic remedy of bathing:
“The aforesaid applies in general. But if one sees that here is possibility of danger unless he is bathed after circumcision, then it is certainly permitted to bathe him and violate Shabbat for his benefit as with any other endangered patient.”
These last words of R. Isserles present us with an additional challenge: What is the dangerous condition which can be diagnosed through mere observation? What such condition can be treated by bathing in hot water?
Four Questions
Let us summarize the four main questions that have been proposed until now:
1. What is the danger which Metzitza is meant to eliminate and what is the medical mechanism which explains this process?
2. What is the purpose of bathing the newborn in warm water after circumcision and again on the third day after circumcision? What is the danger which bathing is supposed to eliminate and what is the physiological mechanism which supports bathing in hot water?
3. Why is the medical indication of bathing after circumcision not absolute and why does it change according to the newborn’s location? What is the location dependent danger to the newborn which requires bathing in hot water after circumcision?
4. What dangerous condition can be diagnosed by visual inspection of the circumcised baby and treated by bathing him in warm water?
A Physician’s Testimony in the Jerusalem district Court
Gonen, M.D., surgeon and mohel, gave expert testimony in Jerusalem District Court during the winter of 1998. In the course of his testimony he described an interesting case which occurred following a circumcision which he had performed around 25 years ago. Dr. Gonen’s story, which constitutes a small part of the court record from the Jerusalem District Court,’7 provides us with a key to solve our little mysteries:
“There was a case that happened in 1980 when I performed a circumcision on a baby who, upon first examination, was normal, without any sign of hypospadias. Immediately following the procedure, I identified that he did in fact have hypospadias, so I did not leave any bandages on him. After 24 hours when I examined him, his glans penis had a bluish- gray color, which is a cause for much concern. This improved after I soaked the baby in a warm water for 40 minutes. This is a technique that encourages dilation of the arteries, so there will be a freer blood flow. I instructed the parents to continue this same treatment six times a day. On my next visit, the baby’s symptoms were gone.”
Dr. Gonen’s story provides a simple, valid medical explanation for R. Moshe Isserles’ opinion. There are cases where the supply of blood to the glans is reduced following a circumcision.’8 Reduction of the supply of blood to the glans is liable to cause an ischemic hypoxia (lack of oxygen) in the glans tissue, which eventually results in gangrene (necrosis) of the glans. Untreated gangrene can then become infected and spread to the body of the penis and eventually endanger the life of the newborn. The primary stage in the pathological process is hypoxia and can easily be identified by simple visual inspection of the glans. The normal rose-like color changes to a bluish- gray, which later on becomes black (signaling gangrene). Soaking the baby in time in warm water indeed dilates the arteries supplying the glans and increases blood flow thus hopefully rectifying the hypoxia. The immediate result of this treatment is: the glans returns to its normal color and all cause for alarm recedes.
After a circumcision, the baby develops a progressing edema (swelling) of the penile tissue, [51] [52] which can reach its apogee on the third day following the surgery. The swelled penile tissue increases the glanular intercellular pressure, almost acting like a tourniquet on the walls of the penile blood vessels, which can lessen their blood flow and eventually lead to hypoxia. Thus, it is understandable from a pathophysiological perspective that the baby most commonly develops an impaired blood flow 24 – 72 hours postcircumcision.
Now the solution to our fourth question, regarding the position of R. Moshe Isserles, is quite evident. What dangerous condition can be diagnosed by visual examination of the circumcised infant and treated by bathing in warm water? The answer is: hypoxia of the glans penis.
We have yet to answer the question why in certain locations there should be a medical indication to bathe all circumcised infants even before diagnosing symptoms of hypoxia. Could there be some places where the danger of hypoxia is more common, thus requiring prophylactic treatment of all circumcised newborns?
To better understand this matter, the next two sections will present the anatomy of a normal penis and then discuss a common penile congenital anomaly.
Anatomy of the Penis
A cross section of a normal penis can be found in textbooks of anatomy[53] and in atlases of human anatomy.[54] On its dorsal aspect (which faces the upper body – the upper portion of the picture in Fig. f) there are the two dorsal arteries which are underneath the overlying layer of skin. These continue on into the dorsal aspect of the glans. Right before entering the glans, each dorsal artery bifurcates into two arterioles: One branch is the artery supplying the glans, and the other branch is the artery supplying blood to the foreskin.
The lower portion of the cross-section shows the elliptical corpus spongiosum, which in its center houses the urethra, which is used to expel both the urine and the semen at the appropriate time. The corpus spongiosum acts as a protective padding along the entire length of the urethra, including the distal portion of the penis, when the corpus spongiosum expands and comprises the entire tissue of the glans.
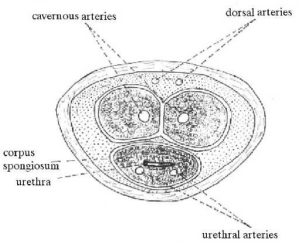
Illustration 1 Normal Penile Arteries Transverse Section of the Penis.
Illustrated by Dr. M. Halperin, following Sobotta Atlas of Human Anatomy, 11th English Edition (Urban & Schwarzenberg, Baltimore-Munich, 1990), vol. 2, fig. 338.
Within the corpus spongiousm, ventral to the urethra, there are the urethral arteries, which supply blood to the corpus spongiosum, the urethra, and the glans.
To summarize, the glans has a blood supply from two pairs of arteries: the dorsal arteries of the penis and the urethral arteries. The urethral arteries are very well protected and reinforced by the corpus spongiosum. The dorsal arteries, on the other hand, are situated at a fairly superficial level, without any padding like the corpus spongiosum. Therefore, they are more vulnerable to trauma induced occlusion, especially following an injury to the penis. Surgical procedures like removal of the foreskin can cause short-term occlusion or even long-term (lasting for days) occlusion in these blood vessels. This is not only due to the swelling and increased pressure in the penile tissue, but it also may result from the local immediate reaction that occurs after cutting the arteries of the foreskin during the surgery. When an artery is cut or lacerated, the arterial walls contract and thus block, or at least decrease, the blood flow. The contraction is a nervous reflex, but it spreads primarily due to a local reaction of the smooth muscle, which seems to cause an action potential that travels a few centimeters along the arterial wall.[55]
When there is a surgical incision of the arteries of the foreskin, which have already branched off from the dorsal arteries, this local reaction that contracts and occludes the arteries can spread to the dorsal arteries in the area before their bifurcation, thus affecting the blood supply of the glans. However, if such a blockage occurs, it has no effect on the alternative blood supply of the glans via the well-padded urethral arteries.
A real problem in blood supply to the glans is liable to occur in newborns with congenital anomalies of the arteries supplying to the glans. Among such anomalies are missing or damaged urethral arteries. In such cases the supply of blood to the glans depends almost entirely on the dorsal arteries. Post circumcision, if the dorsal arteries become even temporarily occluded due to the trauma of surgery, the glans is liable to suffer hypoxia which can lead to necrosis which is a lifethreatening situation for the newborn.
Hypospadias
Hypospadias is the most common congenital anomaly of the penis.[56] The anomaly is expressed by the pathological location of the urethral orifice. Instead of being located as usual at the centre of the glans, in cases of hypospadias the orifice is located more ventrally (lower). In a mild case, the urethra is still located in the glans, but it opens below the center. In more severe cases of penile hypospadias, the opening is placed in the shaft of the penis, between the glans and the scrotum. And, in the most extreme cases, the urethral opening is in the area of the scrotum.[57]
In penile hypospadias, when the urethral opening is located on the ventral aspect of the penile shaft, there are significant structural differences in the area distal to the urethral opening, as compared to the area proximal to it. Before the urethral opening, the penis has, more or less, a normal structure. However, after the opening, the anatomy becomes abnormal. Firstly, the urethra is not present, since it has already opened onto the surface. It is also missing those structures that are always found ventral to the urethra. Thus, the ventral portion of the corpus spongiosum is missing, and sometimes the urethral arteries are missing as well, especially if there were no branches given off that remained in the anomalous portion of the penis (see fig. 2).
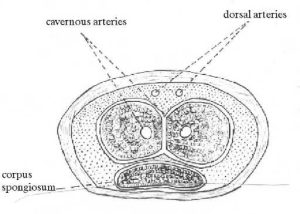
Illustration 2 Penile Arteries in cases of Hypospadias Schematic Illustration of Transverse Section of the Penis, Distal to the Urethral Orifice
Illustration by Dr. M. Halperin
The lack of urethral arteries due to penile hypospadias creates a situation where the glans has an impaired blood supply. It must depend almost exclusively on the dorsal arteries for perfusion. In such a case, were there even a temporary blockage in the dorsal arteries, due to a rising external
pressure or the trauma of the circumcision, the glans can end up having a compromised blood supply (hypoxia),[58] [59] [60] [61] which can develop into necrosis that will endanger the newborn’s penis and even his life.
Therefore, every circumcision on someone with penile hypospadias calls for an extra degree of caution. When the mohel recognizes hypospadias after performing the circumcision and specifically in the cases where the urethra opens on the shaft of the penis directly proximal to the glans, the mohel must be very cautious with any tight bandages. Normally, the bandage won’t occlude the urethral arteries, but in this case if the bandage occludes the superficial and unprotected dorsal arteries, the glans can become severely hypoxic. This is the reason Dr. Gonen mentioned in his testimony: “Immediately following the procedure, I identified that he did in fact have hypospadias, so I did not leave any bandages on him.”
In addition, Dr. Gonen stated that the status of oxygenation of the glans has to be strictly monitored, so any progressing hypoxia (which can develop even without a bandage) can be identified and treated in time. The treatment of choice in such hypoxia is bathing the baby in warm water, as explained in the Mishna, Talmud, comment of R. Moshe Isserles and as described by Dr. Gonen in his testimony.
The Solution of the Mystery of Bathing in Warm Water
Incidence of hypospadias varies in the general population from place to place.6'’ We can therefore justifiably assume that in a location where hypospadias is common, bathing in warm water after circumcision is medically indicated as a prophylaxis for hypoxia of the glans. This indication is absolute in a location where there is a high incidence of penile hypospadias or penile/glans hypospadias hidden by a complete prepuce. In these locations there would be a significant threat that the hypospadias will not be identified on some infants, even after the circumcision. Therefore, without the proper prophylactic care of soaking all circumcised babies in warm water, there would be a high probability of developing necrosis of the glans in some circumcised babies.
In the literature we enlightening regarding the high frequency of hypospadias with complete prepuce (!) in Baghdad over 100 years ago. The report originates with none other than Rabbi Yosef Hayyim, the Chief Rabbi of Iraq, known as ‘Ben Ish Hay’ 6 In his responsa Rav Pe’alim6'1 he wrote:
“For here in Baghdad many such men are to be found whose urethral orifice is below the point where the penis joins the corona (glans), and the mohel examines them and identifies their defect at the time of circumcision and all of them are healthy and fertile. There are men to be found whose sons are also thus. My brother, who is the mohel of our city and who circumcises three quarters of the newborns, told me that around 150 children per year are thus. One of them has fathered many children, all of whom are thus. My brother told me that he senses them at the moment of circumcision. Therefore, the matter is clear and free of concern… it is confounding how the cities of Eastern Europe are fairly unfamiliar with this phenomenon,[62] while here it is a common occurrence.”
In Rabbi Yosef Hayyim’s description there are a number of interesting medical and epidemiological points which call for attention.
First, this is a living description of hypospadias which was discovered ‘at the moment of circumcision,’ but not before. ‘Ordinary’ hypospadias with incomplete prepuce is discovered by simple visual inspection not later than at the preliminary examination performed by the mohel. Hypospadias with complete prepuce, on the other hand, can only be diagnosed at the circumcision unless special painful tests are performed prior to circumcision.
Second, the report described familial distal penile hypospadias with complete prepuce where the orifice is not located in the glans, but in the shaft of the penis “in the place where the penis connects to the glans.”
Third, this is an epidemiological description of an area with a high occurrence of penile hypospadias. In the second half of the 19th century, the Jewish population of Baghdad increased from approx. 20,000 to approx. 40,000.[63] With an occurrence of hypospadias of 200 per year[64] in this population during its period of growth, the direct implication is an astounding 15%-25% occurrence rate of hypospadias, compare this with the 1% occurrence rate in America today.[65]
A medical journal article published in the summer of 1999[66] discusses the hereditary component of hypospadias. The article describes the differences in frequency and severity of hypospadias in two areas of Britain: Portsmouth and Southampton. The single etiology that was found to account for the disparity was a positive family history of hypospadias, which supports the notion of a polygenic mode of inheritance for this anomaly. This conclusion is reminiscent of Rabbi Yosef Chaim’s findings over 100 years earlier, where he describes familial hypospadias to be rare in one geographic location (Western Ukraine) and much more common in another (Babylonia).
The high incidence of penile hypospadias with a complete
foreskin in Babylonia not only provides a very convincing explanation for the approach of Maimonides: “In a place where the practice is to bath a newborn, one ought bathe him before and after the circumcision [even] on Shabbat … because of the danger to the child”, but it also clarifies the motive behind the decisiveness of the ruling of the Babylonian Talmud:[67] The halacha is in accord with Rabbi Elazar ben Azarya in respect to both hot water heated on Shabbat and hot water heated before Shabbat, whether for bathing the whole body or for bathing the area of circumcision, because [not bathing him] it is dangerous for him.” Similarly we find Iraqi Rabbis quoted in the Palestinian Talmud: “Rabbi Yosi bar Bon in the name of ‘the Rabbis from over there’ said that one heats water for the circumcised baby on Shabbat.” This opinion is based on the fact that in locations where there is a high incidence of newborns with penile hypospadias with complete prepuce there is a distinct danger that the hypospadias will not be
identified until after the circumcision. Without prophylactically treating all newborns by soaking in warm water there would be a reasonable probability of developing necrosis of the glans in some of the circumcised babies.
In other words, one might say that Rabbi Yosef Hayyim, the Ben Ish Chai, together with the testimony of Dr. Gonen have given us the key to unlocking the mysteries of the laws governing bathing in warm water as presented above in sections 7-10.
Post-Circumcision Hypoxia in Israel
It is important to emphasise that spontaneous hypoxia of the glans following circumcision, even if it is to be expected more often in babies with penile hypospadias, is not unique to such babies. Arterial blood supply to the tissues of the penis is not consistent throughout the population.
Angiographic imaging of the pudendal artery, which supplies blood to the penile arteries, has shown a wide variation in the distribution of the penile arteries in normal men.[68] [69] Certain variations in such distribution can alter the scope of potential alternate paths in blood supply to the glans, which can also put some males at higher risk for post-circumcision hypoxia.
Therefore, even these “normal” males can end up developing spontaneous post-circumcision hypoxia of the glans, which supports the medical indication for bathing all circumcised males in warm water, as explained above.
Medical knowledge regarding hypoxia following circumcision exists, as stated above, in the halachic literature. Most of this knowledge is still lacking in contemporary medical literature.
This results in omitting this important information when physicians provide medical training for mohalim^ Further, there are even many traditionally trained mohalim who have never been briefed on the subject of soaking in warm water as a prophylactic treatment for post-circumcision hypoxia.[70] The inevitable result is the relatively rare phenomenon of hypoxia following circumcision. Such hypoxia could have been prevented by soaking the babies in warm water in accord with the ruling of the Mishnah and the Babylonian Talmud.
During the last decade there have been in Israel a number of cases of necrosis of the glans at 3-10 days after circumcision. In all these cases the circumcision was performed by highly experienced mohalim. Careful study of these cases indicates a high probability that they were caused by postcircumcision hypoxia. Such hypoxia could have been prevented by soaking the babies in warm water after the circumcision and on the third day following. Surely soaking in warm water immediately upon discovery of the initial symptoms of hypoxia could have prevented the development of necrosis. But lack of knowledge, both on the part of the physicians who examined the babies and by the mohalim, impeded the correct medical treatment in these cases.
Erroneous Medical Reports
A review of the medical reports submitted to the courts for these previously mentioned cases shows their explanations are insufficient. It seems that the physicians who wrote the opinions are not adequately familiar with spontaneous postcircumcision hypoxia. As a result, they attempted to assemble various medical explanations for its occurrence, which might politely be called unconvincing.
Let us consider two characteristic cases:
Case one: D., the son of couple A, was circumcised on the afternoon of the eighth day, 25 January 1992, falling on a Shabbat. Later that day the mohel called and asked whether all was well and whether the baby was urinating. The following day the mohel visited and removed the bandage. Mrs. A., the baby’s mother, remembers that when the bandage was removed the penis looked ‘normal and pink.’ At least six or seven hours later, the colour of the penis changed and the change became more pronounced the next day. Two days after the circumcision the staff at the municipal infant-care centre referred the mother to a peadiatrician who in turn referred the baby to a hospital. One more day passed until the baby was brought to the hospital. Even in the hospital they apparently failed to soak the baby in warm water. The day following his admission to the hospital, the tip of the glans was already black. Ten days later, the black portion of the glans was sloughed off.[71]
Criminal charges (!) were based, in part, on the expert opinion of Dr. A.A., a plastic surgeon from the central part of Israel. His opinion was based on an interview with the parents, an examination of the baby a year and a half after the circumcision, and four documents: the birth report, the patient’s admission form, discharge form, and the referral written to the plastic surgery clinic. In analysing the factors for the sloughing off of the glans, he wrote[72] that “it seems the cause is concealed within one of two possibilities:
1. Excision of part of the glans during the circumcision and subsequent necrosis of the rest.
2. Bandaging after the circumcision caused pressure which impeded the blood supply to the tip of the penis, resulting in the development of necrosis.
In my opinion, the second reason is more likely.”
In light of the agreed data in this case, it is clear that neither of the two reasons are acceptable. Both the mohel and the mother testified that after removing the bandage on the day after the circumcision ‘the penis looked “normal and pink.”[73] It is also agreed that the infant urinated without difficulty or discomfort. It is further agreed that the change in the skin colour of the glans did not occur when the glans was bandaged, but rather many hours later. Therefore, neither of the two proposed reasons is at all likely. They were certainly proposed in only out of the doctor’s lack of awareness of any better explanation.
It seems to us that the data quoted above regarding the phenomenon of “spontaneous postcircumcision hypoxia” clearly explain both the phenomenon itself, the methods of prophylaxis, and the required preliminary medical treatment.
Case two: This case was brought as a civil lawsuit in Jerusalem.[74] Baby R.A. was circumcised on the eighth day, on a Sunday afternoon before the beginning of the Festival of Shavuot, on 15 May 1994. It is agreed that he was examined around one half hour later by the mohel who changed the bandage. The baby urinated without problem and without any signs of discomfort. Being familiar with the traditions of the Shulchan Aruch, the mohel did not instruct the parents to bathe the baby in warm water. The mohel removed the bandage on the evening following the festival, and examined the baby again on Tuesday evening. The last examination was performed by the mohel on Wednesday night, three days after the circumcision. At that examination the mohel saw the beginning of blackening of the glans.[75] The baby was brought to emergency room after another day and a half, on Friday morning. At that time he was diagnosed a suffering from dry gangrene of the glans and was sent home without any further treatment and without any recommendation of bathing in warm water. After one more day, when the condition of the penis deteriorated further, the baby was rushed again to hospital, treated with a broad spectrum antibiotic. After several hours, the distal end of his penis sloughed off.
The baby’s parents sued the mohel for civil damages, claiming that tight bandaging on the day of the circumcision had caused the necrosis.
Expert medical testimony which was appended to the law suit and supported the parents’ claim had to deal with the fact that after the circumcision and prior to removal of the bandage the infant urinated normally and without any symptoms of distress. Such urination has never been described, and probably is impossible, if the bandage is tight enough to prevent an arterial blood flow. The court also received contradictory evidence and documents regarding the infant’s penile hypospadias[82] hidden by a complete foreskin.
Dr. A.L., an urologist from central Israel, was called as a witness by the plaintiff. In his opinion he wrote:
“Necrosis of the penis is caused when the blood supply is compromised. A number of conditions are liable to cause this, including severe trauma, major infection, and pressure. In this case there is no documentation pointing to any cause which might have caused an acute impediment in the blood supply to the penis except for the pressure of the bandage which had been applied to stop bleeding.”
Dr. A.L. did not deal with the fact that there was no evidence of excessive pressure in the bandage and that the infant urinated without any symptoms of distress over an entire day whilst it was so bandaged. From Dr A.L.’s testimony, it seems as though he was unfamiliar with the data described in the previous sections regarding the phenomenon of “spontaneous post-circumcision hypoxia.” These data can indeed give a very good explanation for how this baby’s hypoxia occurred. In addition, they give the necessary preventative measures and medical care that should have been administered.
Dr. Y.L from Jerusalem is a general surgeon and urological surgeon who also contributed his opinion for the plaintiffs. He too was unfamiliar with the phenomenon of “spontaneous postcircumcision hypoxia,” and as a result he was compelled to link the necrosis to the tightness of the bandage, despite the fact that the baby urinated without complication and without any signs of discomfort. In addressing the conflicting testimonies over whether the baby was actually suffering from hypospadias, he referred to[83] a Paediatric Urology article from 1991, which did not find “any reference to significant impediment in blood supply to the glans in cases of hypospadias.”
Taking into account that the medical literature did not report its first case of defective glans blood supply until 1995, Dr. Y.L.’s cited article was simply not current enough. This is why Dr. I.H., an expert urologist from London who submitted his opinion for the defendants, wrote that newborns with hypospadias can have significant disruption in glanular blood supply. His claims relied on anatomical changes in hypospadias as well as on an up-to-date opinion (1998) of a well-known British specialists in paediatric urology in Britain leading to the conclusion, that there is indeed a possibility
of significant impediment to the blood supply to the glans in newborns suffering from hypospadias.
Further, in light of the lessons learned in the history of medicine and from the development of medical science in the field of circumcision, one might expect that several more years might be required until data currently to be found only in the religious literature of mohalim find their way into medical literature. This has indeed come to pass, as indicated in section 3-5 above.84
One factor which may accelerate this important process is the medical and technical expertise of experienced physicians who are well-trained in the halachic performance of Brit Milah on newborns. They have the means to play a key role in advancing this process due to their expert training in modern medicine combined with a depth of knowledge of the halachic works dealing with Brit Milah. Dr. Gonen’s testimony is thus not simply a routine legal document. It is rather the first medical source to mention the existence of and initial treatment of “spontaneous post-circumcision hypoxia,” a phenomenon more common amongst newborns with penile hypospadias, but which also happens in lesser incidence to normal newborns.
The Legal Significance
Jurist dealing with these matters require more than superficial popular knowledge. Special training in medicine, halacha, and law must be offered in order to enable deeper understanding of [84] [85] medical topics which arise in courts of law. We would not be surprised if in the future someone who is ignorant of proper understanding and who nevertheless presents to the court complicated medical matters might be guilty of professional malpractice.
Experience has shown that courts of law view themselves as possessing authority over those who appear before them. Unfortunately, the courts do not always possess the tools required to decide cases subject to professional controversy. It is natural in such cases that witnesses fail to disclose their limitations to the court. This requires that the court exercise caution and employ their common sense, which should in some measure enable them to determine existing professional limitations. This is all the more so when legal deliberations take place at the same time that medical science is developing in the area under deliberation, and a decision must be taken before a professional international consensus can be ascertained.
Progress in medical science touching upon “spontaneous post-circumcision hypoxia of the glans” is a current example of erroneous opinion expressed by expert witnesses and consequent perversion of justice.
The Medico-halachic Significance
I have spoken with a number of experienced mohalim, among them the last mentioned mohel. They had been trained by their teachers to perform a circumcision according to the Rabbi Yosef Karo, the author of the Shulchan Aruch. Therefore, they did not learn about bathing the baby in warm water after circumcision even on weekdays. Pursuant to my recommendation they have begun to instruct parents of circumcised babies to bathe them in warm water beginning the day after the circumcision. They all report that since instituting this bathing, the circumcised baby’s penis was healing significantly faster.
Israel has attracted Jews from all over the world, both from places and families where bathing in hot water is vital in preventing danger and from places where such danger is rare. In light of the clinical experience which has accrued in this area, it seems to me that in the State of Israel we are obligated to insist on bathing in warm water after every circumcision. Similarly, when training mohalim, it would be proper to teach them this medico-halachic subject and the practical ramifications which flow from it.
The Solution of the Mystery of Metzitza:
Why Metzitza was instituted
Immediately after incising or injuring an artery, the arterial walls contract and occlude, or at least reduce, continued flow of blood. The constriction is caused in part by a nervous reflex and principally by a local reaction of the smooth muscle layer of the artery. This apparently leads to induction of an action potential (resulting in contraction) that can travel along several centimetres of the arterial wall.8'’ Excising the prepuce can, therefore, cause a temporary occlusion in the dorsal arteries as a result of the localised reaction to the incision of the arterioles of the prepuce as these branch off of the dorsal arteries.[86] [87]
This transient arterial occlusion caused by muscle contraction continues to develop into a more enduring blockage as the hindered and stationary blood begins to clot. The primary stage in the pathological process is hypoxia which can easily be identified by simple visual inspection of the glans without any need to be familiar with the knowledge of modern medicine. Only an immediate resolution of that occlusion can stymie the local process of coagulation, which can turn the transiently occluded artery into a permanently blocked artery. Indeed, were this artery to become fully obstructed and no longer supply the glans with blood, it would generally have no effect on the alternative blood supply of the glans, which comes from the well-protected and padded urethral arteries. However, in those instances where a congenital anomaly affects the urethral arteries, a transient blockage of the dorsal arteries can cause severe hypoxia of the glans. If the arterial obstruction becomes more permanent, the baby may lose his glans and it may even become a lifethreatening situation.
Performing Metzitza immediately after circumcision, on the other hand, lowers the internal pressure within the tissues and blood vessels of the glans, thus raising the pressure gradient between the blood vessels at the base of the penis and blood vessels at its distal end – the glans as well as the excised arterioles of the prepuce which branch off of the dorsal arteries.
This increase in pressure gradient (by a factor of 4 to 6!) can resolve an acute temporary occlusion and restore blood flow to the glans, thus significantly reducing both the danger of immediate, acute hypoxia and the danger of developing a permanent obstruction by means of coagulation.
The indication that the temporary occlusion has been resolved is that “the blood in the further reaches (= the proximal dorsal artery) will be extracted” as Maimonides has stated.87
It is therefore clear that the claim of the Sages and the halachic authorities that Metzitza can prevent danger to the baby is in exact agreement with the most up-to-date medical science. Metzitza, like bathing in warm water, plays an important role in minimising the risks associated with circumcision. Today we understand the mechanisms by which these halachot accomplish their purpose. This is especially so in light of the lessons learned in cases of necrosis of the glans as described above.
With this clearer understanding of the basis for these laws, it is advisable to analyze anew the words of the rishonim, the mediaeval commentaries. Reexamination of the commentary of Rabbi
Yaakov Hagozer[88] shows his explanations have a surprising consonance with this contemporary medical explanation:
“Metzitza… How? After the incision and splitting the membrane, one immediately brings the penis into his mouth and sucks out blood with all one’s strength, because if he does not suck, the blood will clot in the top[89] of the penis and this is dangerous.[90] It is similarly said in chapter Rabbi Eliezer [the 19th chapter otMasechet Shabbat]: ‘Rav Pappa said: A mohel who does not perform Metzitza endangers the baby and is dismissed’ because the blood will clot within the penis and this is dangerous.[91]”
In summary, we can say that in light of the clinical lessons learned over the last few years from cases of post-circumcision hypoxia of the glans and in light of modern anatomy and pathophysiology, we have finally rediscovered the medical reason for Metzitza and verified that the words of the Sages are literally correct.
The Hebrew term ‘atarah’ means glans penis. Dr A.M. Mazia in his Sefer ha-Munachim le-Refu’ah u-le-madda’ei ha-Teva, Jerusalem, 5694; See Beit Yosef Y.D. 264 regarding the question of the Spanish authorities in this matter; cf. commentaries ad loc.; Rav Yosef Kafih on Hilchot Mila 2:6.
I Wiswell Thomas E., “Circumcion Circumspection” XI JM April 24, 1997; 336(17):1244-1245.
II Sharon Bass (Deputy Editor), “Circumcision persists despite doctors’ disapproval”, Maine Times, January 1997, Vol. 29 No. 9.
[1] Shabbat 133b.
[2] Sections 3-5 above.
[3] Shulchan Aruch Orach Chaim 331:9
[4] Niku SD, et al., “Neonatal circumcision” Urol Clin North Am 1995 Feb; 22(l):57-65.
[5] ibid.
[6] Shabbat 19:2-3 and the corresponding Talmudic passages and commentaries.
[7] Maimonides, Hilchot Rotseach 1:18.
[8] Maimonides, Hilchot Yesodei ha-Torah 5.
[9] Yalkut Shimoni, Yitro 292 and Va-Yikra Rabba (Vilna ed.) 32 .s!.v. va- yetsei ben.
[10] “In England, the Royal House has a long tradition requiring that all male children be circumcised by the Jewish “mohel” of London.” Alfred J. Kolatach’s The Jewish Book of Why (Middle Village, New York; Jonathan David, 1981).
[11] https://funspot.net/malka
[12] Harrison’s Principles of Internal medicine, 14U1 edition (1998) p. 737.
[13] Y.L. Katzenelsohn, Ha-Talmud ve-Chochmat ha-Refuah, (pub. “Chayim”, Berlin, 1928), p. 277.
[14] Otto JC, Med Respiratory 6:1, 1803. Cited in: Rosner F, Ann Intern Med 70:833, 1969; Steinberg, Enc. Hilchatit Refu’it 3 (Schlesinger Inst., Jerusalem, 5752), 5.1׳. mila, note 459.
[15] Yevamot 64b.
[16] Maimonides, Hilchot Mila 1 at end.
[17] Beit ha-Behira on Yevamot 64b.
[18] Notes on Yoreh Deah 263:2.
[19] Y.L. Katzenelsohn, Ha-Talmud ve-Chochmat ha-Refuah, pp. 231226.
[20] Julius Preuss, Biblical and Talmudic Medicine, (Translated and edited by Fred Rosner, Hebrew Publishing Company, New York, 1978) p. 245.
[21] Babylonian Talmud, Yevamot 64b
[22] Ctenturies later there were rabbis who, due to absence of a detailed explanation of this halacha (which today we know to be based on inherited haemophilia), followed the medical science known in their time and therefore tended to equate males and females. For example, Rabbenu Manoach, quoted in Beit Yosef Y.D. 263.
[23] A description of the anatomy, pathology and pathophysiology of hypospadias is discussed in Section 13 below.
[24] Hatch DA, Maizels M, Zaontz MR, Firlit CF, Hypospadias hidden by a complete prepuce, Surg Gynecol Obstet 1989 Sep;169(3):233-4.
[25] R. Yosef Hayyitn (Ben Ish Hay), Resp. Rav Pe’alim, Even ha-Ezer, 111:12. See section 14 below.
[26] M. Shochat and Sh. Ashkenazi, Refu’at Yeladim, 3rd. ed., Pt. 1, pp. 121-123.
[27] There can be other causes for newborn jaundice, which include completely different pathologies or the common occurrence of physiologic jaundice, where a developmentally delayed liver is unable to excrete the normal amount of plasma bilirubin during the first few days after birth.
[28] Shabbat 134a.
[29] Levy Yaakov in Noam 10,168-179 (1967).
[30] ‘yarok’ in many Talmudic passages means ‘yellow.’ Cf., for example, Brachot 25a and Rashi s.v. holi she-shemo galintsa, and Otsar Lo’azei Rashi by R.M. Catane, no. 18. SeeAruch ha-Shalem s.v. ירק.
[31] Shabbat 19:2.
[32] A mohel who lived during the first half of the thirteenth century (Ya’akov Segel Glasburg Hamohel, Shochet U’Bodek D’Kahal Kadosh Berlin, in the Introduction of SeferZichron Brit L’Rishonim, Berlin 5652, Photocopied version: Jerusalem, 5732, p. VIII.)
[33] Zichron Brit L’Rishonim (ibid), p. 20.
[34] Hilchot Mila, chapter 2.
[35] Viz. ‘or medicinal powder which staunches the blood,’ Shulchan Amch, Y.D. 264:3.
[36] ibid.
[37] ChochmatAdam 149:14.
[38] In the absence of any clear tradition regarding the nature of the danger which Metzitza is meant to prevent there have been many suggestions and opinions. See Sedei Hemed, Millu’im le-qunt. ha- Metzitza׳, Rav M.B. Pirutinski, Sefer ha-Brit (New York, 5733), sect. 264:7; Rav A. Cahn, Brit Avraham ha-Kohen on Rabbenu Yaavats— Hilchot Mila (Brooklyn, 5744), pp. 190-191; A. Steinberg, Enc. Hilchatit Refu’it 3, s.v. Mila.
[39] Rav Kuk, Daat Kohen, 140-142; Brit Avraham ha-Kohen, pp. 191192; Tiferet Yisrael ad Shabbat 19:2.
[40] Rav S.R. Hirsch, Resp. Shemesh Maipe, 44-45, quoted in Brit Avraham ha-Kohen, pp. 194-195.
[41] R. Yitshak bar Sheshet, Response, 447.
[42] ibid.
[43] Avraham Steinberg, preface to Perakim B’Patologia B’Talmud Uv’Nosei Keilav, Sefer Assia 6,193-198.
- Ignaz Philipp Semmelweis, 1818-1865.
[45] Rav S.R. Hirsch, Resp. Shemesh Maipe, ibid. Rav A.A. Gruenwald, Zocher ha-Brit 12:31.
[46] Zocherha-Brit 11:18-19.
[47] Rav S.R. Hirsch, Resp. Shemesh Maipe 55, quoted in Brit Avraham ha-Kohen, pp. 191-192; Rav Kuk, Daat Kohen, 140-142.
[48] Shabbat, 19:3.
[49] Jerusalem District Court, Case 001013/96; court record of 9 March 1998, p. 82.
[50] In principle in accord with Tosafot Rid, Shabbat, ibid., where Shibbolei ha-Leket, Hilchot Mila 2 is also quoted. A similar practice was instituted by Rabbi Yaakov ha-Gozer, ibid., p. 33. After quoting the Talmudic passage and the commentators, he wrote: ‘Therefore our rabbis permit making a fire to heat water and prepare all that is necessary for circumcision on Shabbat which falls within the first three days. One proceeds just as during a weekday whenever he is not strong.’ He added: ‘I too have instituted the bathing of the baby on the third day which falls on Shabbat in the same warm water which was heated before Shabbat. Delaying the bath until Saturday night is a strict position which I do not accept unless there is clearly no danger.’
[52] Such cases are more common in babies with congenital hypospadias, as indicated by Dr Gonen when he mentioned discovering hypospadias after circumcision and his consequent decision not to bandage the baby. Relevant physiological and anatomical explanations can be found below in sections 12-13.
[53] See Gray’s Anatomy, 35lh edition, Pub. Longman 1973, pp. 670; 1347-1348.
[54] See Sobotta Atlas of Human Anatomy, lllh English Edition (Urban & Schwarzenberg, Baltimore-Munich, 1990), vol.2, fig. 338.
[55] See Guyton A.C., Textbook of Medical Physiology, 5lh edition, (W.B. Saunders Co., Philadelphia, 1976), p. 99.
[56] Nelston Textbook of Pediatrics, 12lh edition (W.B. Saunders Co., Philadelphia 1983) p. 1392.
[57] ibid.
[58] A further anomaly in blood supply to the glans occurs in newborns suffering from hypospadias with complete prepuce, see:
Persad R, Sharma S, McTavish C, Imber C, Mouriquand PDE, Clinical presentation and pathophysiology of meatal stenosis following circumcision, British Journal of Urology, 1995; 75:91-93.
[59] The incidence of this defect in the western world varies from place to place and effects between 1 and 8 newborns per thousand (a factor of 800%!). See:
Neslon Textbook of Pediatrics, ibid•, Harrison’s Principles of Internal Medicine, 14lh edition, (McGraw-Hill, New York, 1998), vol. II p. 2130.
[60] R. Yosef Hayyim b. Eliyahu was born in Baghdad in 1835 and died in 1911.
[61] Resp. Rav Pe’alim, Even ha-Ezer, 3:12.
[62] R. Yosef Hayyim of Baghdad refers here to a responsum of Resp. Sho’el u-Meishiv III, 1:206, by R. Yosef Shaul Nathansohn (18101875) from Lemberg (Lwow, a city in the Western Ukraine). That responsum considers hypospadias to be something exceedingly rare.
[63] Enc. Ivrit, s.v. Bagdad; Iraq.
[64] 150 cases observed by a mohel who circumcised 75% of the newborns implies around 200 cases in the whole population of circumcised babies.
[65] Harrison’s Principles of Internal Medicine, ibid.
[66] Chambers EL, Malone PS, The incidence of hypospadias in two English cities: a case-control comparison of possible causal factors, BJU Ini 1999 Jul; 84 (1): 95-8.
[67] R. Abbahu in the name of R. Yohanan. Further discussion is beyond the scope of this article.
[68] Bennett Alan H., Impotence – Diagnosis & Management of Erectile Dysfunction. W.B. Saunders Co., Philadelphia, 1994, p. 21.
[69] On 14 Sivan 5737 a national conference of mohalim took place at Shaare Zedek Medical Centre in Jerusalem. The conference was organised by The Schlesinger Institute for Medical-Halachic Research in conjunction with the Inter-ministerial Committee for Supervising Mohalim at the Chief Rabbinate. A summary of the medical lectures was published in a special booklet edited by Dr. Avraham Steinberg and published by the Schlesinger Institute. This material was reprinted in SeferAssia 3:355-392.
[70] Although the practice in Europe generally follows opinion of R. Moshe Isserles, Rabbi Tsvi Binyamin Auerbach from Frankfurt a.M. wrote in his Brit Avraham (page 89; publ. Frankfurt, 1880) that ‘we do not customarily bathe the child before or after circumcision.’ (!)
[71] Source: Magistrates Court in Tel Aviv-Yafo, Criminal Case 4463/96, State of Israel v. Triki, Joseph, decision as of 15 July 1997, pp. 4-5.
[72] Dr A.A., page 2 of the medical opinion dated 22 February 1994.
[73] Decision of the court, ibid.
[74] Civil Case 001013/96 in the Jerusalem district court.
[75] The Court heard contradictory testimony regarding the question whether the blackening was first observed at this examination or earlier.
[82] From the end of the 1980s, the medical literature has recognized the existence of penile hypospadias (on the ventral aspect of the penis) with a fully-formed foreskin. For an example, see: Hatch DA, Maizels M, Zaontz MR, Firlit CF, Hypospadias hidden by a complete prepuce, Surg Gynecol Obstet 1989 Sep;169(3):233-4.
[83] In an undated complementary opinion from January, 1999.
[84] The first study dealing with topic of the anatomical anomalies in hypospadias was first published in the fall of 1998. See: Baskin LS. Erol A. Li YW. Cunha GR. Anatomical studies of hypospadias. Journal of Urology. 160(3 Pt 2): 1108-15. The investigators used a hypospadic penis from a fetus aborted in week 33 to prepare histological slides. They compared their findings to aborted fetuses with ־־normal” penises. The conclusions of the study were: "The most striking difference between the normal and hypospadic penis
[85] the abnormal urethra and glans with respect to vascularity.” This stems from the fundamental difference between a hypospadic penis and a normal penis: the vascular supply of the glans (ibid, page 1112). The article concludes with a declaration for the need to broaden the medical knowledge which is clearly lacking in this area, which will lead to better strategies of care for hypospadias.
[86] Guyton A.C., Textbook of Medical Physiology, 5lh edition, (W.B. Saunders Co., Philadelphia, 1976), p.99.
87. Hilchot Mila, chapter 2.
[87] See section 12 for a discussion of the penile blood supply.
[88] Zichron Brit L’Rishonim, Berlin 5652, page 20.
[89] The “top of the penis” here cannot mean the ‘urethral meatus,’ where doted blood can easily be removed without metzizah. Therefore, the right understanding should be: the ‘blood vessels within the distal parts of the penis.’
[90] My emphasis (M.H.).
[91] My emphasis (M.H.).